How to Increase Vitamin B12 Naturally — Foods, Absorption, and More
Learn how to boost your B12 levels through diet and absorption tips, plus how B12 connects to vitamin D3, folate, and iron.

Maybe you got your blood work back and your B12 is flagged low. Or maybe you’ve been taking a B12 supplement for months and you’re wondering — do I actually still need this pill?
Either way, you’re asking the right question. Vitamin B12 deficiency affects an estimated 6% of adults under 60 and up to 20% of those over 60. And while supplements absolutely have their place, many people can maintain healthy B12 levels through diet alone — if they know what to eat and how to absorb it.
This guide covers the best natural sources of B12, how to maximize absorption, what connects B12 to other vitamins like D3 and folate, and how to safely transition off supplements if that’s your goal.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting or changing any supplement regimen. The dosages and reference ranges below are drawn from published clinical guidelines and are not personal recommendations.
What Is Vitamin B12 and Why Does It Matter?
Vitamin B12 (cobalamin) is a water-soluble vitamin that plays a critical role in several essential body functions:
- Red blood cell formation — B12 is required for healthy red blood cells. Without it, cells become abnormally large and ineffective (megaloblastic anemia).
- Nerve function — it maintains the myelin sheath that protects your nerves. Deficiency can cause tingling, numbness, and even permanent nerve damage if left untreated.
- DNA synthesis — every cell in your body needs B12 to divide properly.
- Homocysteine metabolism — B12 helps convert homocysteine to methionine, which matters for cardiovascular health.
Unlike most water-soluble vitamins, your body stores B12 in significant amounts — about 2 to 5 mg in the liver. This means deficiency develops slowly, often over 3 to 5 years, which is exactly why it’s frequently caught late.
Who’s at Risk?
B12 deficiency isn’t just a vegan problem — though plant-based eaters are the most well-known risk group. You may also be at higher risk if you:
| Risk Factor | Why It Matters |
|---|---|
| Age over 50 | Reduced stomach acid impairs absorption of food-bound B12 |
| Vegan or strict vegetarian | No natural plant sources of B12 exist |
| Taking PPIs or H2 blockers | These reduce the stomach acid needed to release B12 from food |
| Taking metformin | Well-documented to reduce B12 absorption by 10-30% over time |
| GI conditions (Crohn’s, celiac) | Impaired absorption in the terminal ileum |
| Post-bariatric surgery | Permanent changes to digestive anatomy |
| Heavy alcohol use | Damages gastric lining and depletes liver stores |
Common deficiency symptoms include persistent fatigue, tingling or numbness in hands and feet, difficulty with balance, brain fog, low mood, and a swollen or smooth tongue. The neurological symptoms can occur even without anemia — which is why testing matters.
The Best Natural Food Sources of B12
B12 is produced by microorganisms and enters our food supply primarily through animal products. Here are the richest dietary sources:
| Food | Serving | B12 (mcg) | % Daily Value | Source |
|---|---|---|---|---|
| Clams | 3 oz cooked | 84.0 | 3,500% | NIH ODS |
| Beef liver | 3 oz cooked | 70.7 | 2,946% | NIH ODS |
| Sardines | 1 can (92g) | 7.6 | 317% | USDA |
| Rainbow trout | 3 oz cooked | 5.4 | 225% | NIH ODS |
| Sockeye salmon | 3 oz cooked | 4.8 | 200% | NIH ODS |
| Tuna | 3 oz canned | 2.5 | 104% | USDA |
| Beef (lean, ground) | 3 oz cooked | 2.4 | 100% | NIH ODS |
| Milk | 1 cup | 1.2 | 50% | USDA |
| Yogurt | 6 oz | 1.0 | 42% | USDA |
| Eggs | 1 large | 0.6 | 25% | USDA |
Daily Value based on the adult RDA of 2.4 mcg/day.
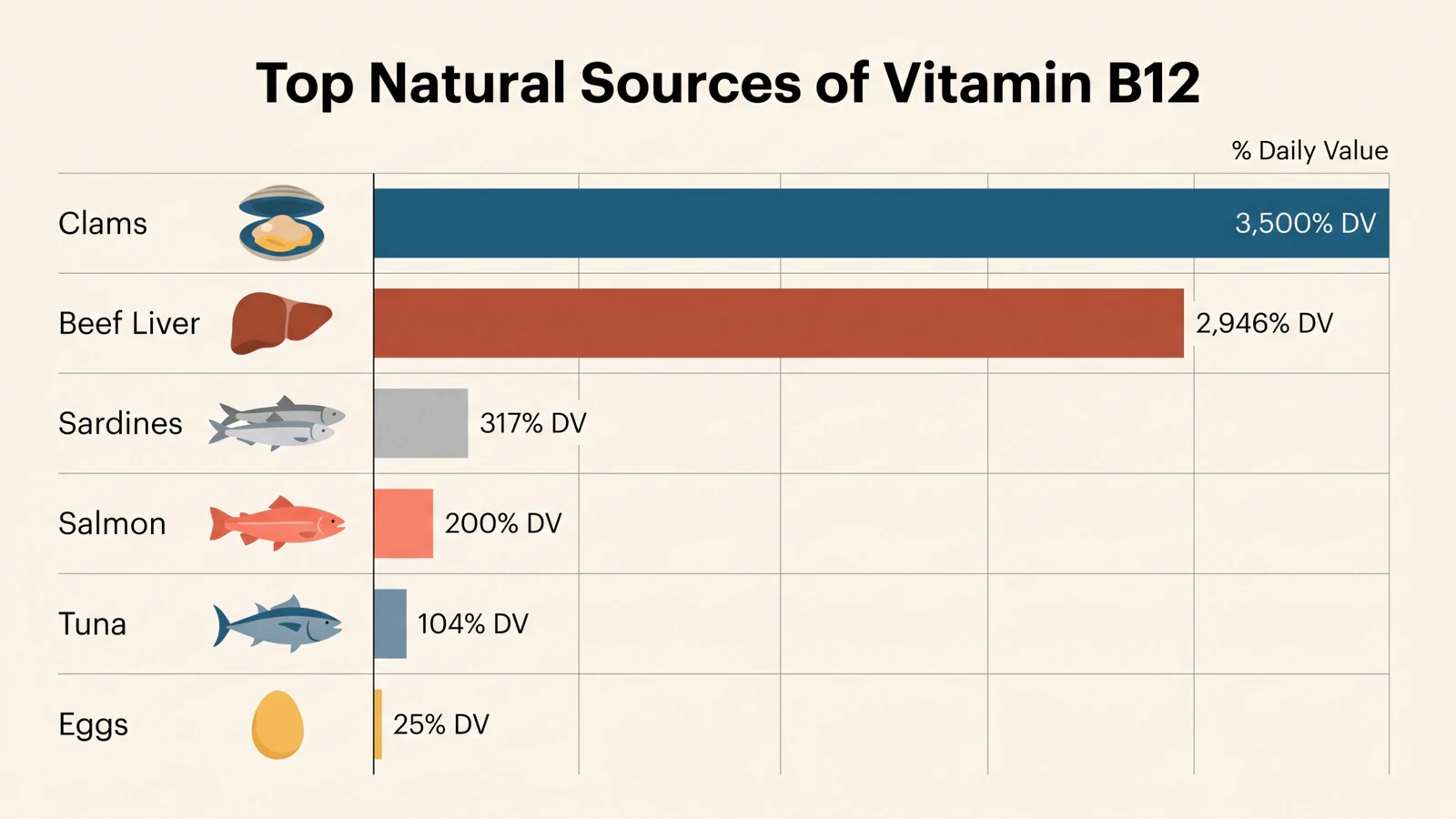
A few things stand out. Shellfish and organ meats are in a league of their own — just 3 ounces of clams delivers over 35 times your daily requirement. Fish is the next best category. Dairy and eggs provide B12, but in smaller amounts — you’d need to be intentional about including them at multiple meals.
A note for plant-based eaters: There are no reliable unfortified plant sources of B12. Spirulina and most algae contain B12 analogues (pseudocobalamin) that your body cannot use — and may actually interfere with true B12 absorption. Fortified foods like nutritional yeast, plant milks, and breakfast cereals are the only viable plant-based option, but these are technically supplemented.
Beyond Diet: Optimizing B12 Absorption
Eating B12-rich foods is only half the equation. Your body needs to actually absorb it — and several factors can quietly get in the way.
Stomach Acid Is Essential
B12 in food is bound to proteins. Your stomach acid breaks those bonds so B12 can attach to intrinsic factor (a protein made in your stomach lining) and be absorbed in the small intestine. Anything that reduces stomach acid — like chronic PPI or H2 blocker use — can impair this process significantly.
If you’re on long-term acid-reducing medication, talk to your doctor about monitoring your B12 levels annually. The NIH recommends that adults over 50 get their B12 primarily from fortified foods or supplements, since age-related decline in stomach acid affects 10-30% of older adults.
Gut Health Matters
B12 is absorbed in the terminal ileum — the last section of the small intestine. Conditions like Crohn’s disease, celiac disease, or small intestinal bacterial overgrowth (SIBO) can impair absorption at this site. If you have a diagnosed GI condition and your B12 is low, dietary changes alone may not be enough.
Watch for Depleters
- Alcohol — even moderate-to-heavy drinking damages the gastric lining and reduces liver stores
- Metformin — if you’re taking it for diabetes, ask your doctor to check B12 at your annual blood work
- Nitrous oxide — recreational use rapidly inactivates B12, which can trigger acute deficiency even in people with normal stores

Common Myths About B12
“Spirulina and algae are great plant sources of B12.” Not quite. Most algae contain pseudocobalamin — a B12 analogue that looks like B12 on a lab test but doesn’t function like it in your body. Nori may contain small amounts of active B12, but the quantity is unreliable and insufficient to prevent deficiency.
“B12 supplements will give you more energy.” Only if you’re actually deficient. B12 is involved in energy metabolism, but supplementing above normal levels doesn’t create a boost. The “energy shot” effect people report from high-dose B12 is either correcting an undiagnosed deficiency or a placebo response.
“A normal serum B12 means you’re fine.” Not always. Serum B12 is an imperfect test. Functional deficiency can exist even with levels in the “normal” range of 200-400 pg/mL. Methylmalonic acid (MMA) is a more sensitive marker — if your B12 is in the gray zone and you have symptoms, ask your doctor about checking MMA.
“Only vegans need to worry about B12.” This is the most common misconception. Studies show that 10-15% of adults over 60 are deficient regardless of diet, thanks to age-related absorption decline, medication use, and GI conditions.
B12’s Connection to Vitamin D3, Folate, and Iron
One thing that surprises many people: nutrient deficiencies rarely travel alone. If your B12 is low, it’s worth checking a few of its closest neighbors.
B12 and Vitamin D3
B12 and vitamin D3 deficiencies frequently co-occur — especially in older adults, people with GI conditions, and those with limited dietary variety. This isn’t because one directly affects the other biochemically, but because they share many of the same risk factors.
Both vitamins are critical for neurological health, and some research suggests that combined deficiency may have compounding effects on cognitive function in older adults. If you’ve been told your B12 is low, it’s worth asking your doctor to check your vitamin D at the same time — and vice versa. (For a deep dive on vitamin D, check out our beginner’s guide to vitamin D deficiency.)
B12 and Folate (B9)
This is the most clinically important interaction. B12 and folate work together in the same metabolic pathway. When B12 is low, folate gets trapped in an unusable form — a phenomenon called the methyl-folate trap. The result? Both deficiencies cause the same type of anemia (megaloblastic), making them hard to distinguish from blood work alone.
Here’s the critical part: high folate intake — from supplements or heavily fortified foods — can mask B12 deficiency by correcting the anemia while neurological damage continues silently. This is why clinicians always recommend checking B12 before treating folate deficiency.
B12 and Iron
B12 deficiency and iron deficiency are the two most common nutritional anemias worldwide, and they can coexist in the same person. When they do, it gets tricky — the large red blood cells from B12 deficiency and the small red blood cells from iron deficiency can cancel each other out on a standard blood test, producing a normal-looking result that hides both problems.
The takeaway: If you’re investigating any kind of anemia or fatigue, ask for the full panel — B12, folate, iron, and ferritin. Testing just one can miss the bigger picture.
Transitioning Off B12 Supplements Safely
If your deficiency was caused by diet and you’ve corrected your eating habits, it’s reasonable to ask: can I stop the supplement? The answer depends on why you were deficient in the first place.
When Stopping May Be Appropriate
- Your deficiency was purely dietary and you’ve shifted to a B12-rich diet
- The medication that was causing depletion has been discontinued
- You have no underlying absorption issues
When Supplements Are Non-Negotiable
- Pernicious anemia — this is an autoimmune condition that destroys intrinsic factor. You’ll need lifelong B12 injections or high-dose oral supplements.
- Post-bariatric surgery — the anatomical changes are permanent.
- Chronic malabsorption disorders — Crohn’s disease affecting the terminal ileum, for example.
- Strict vegans who don’t consistently eat adequate fortified foods.
How to Taper Safely
If your doctor agrees that stopping makes sense, here’s a reasonable approach:
- Get baseline labs — serum B12, methylmalonic acid (MMA), and homocysteine before you change anything
- Build up your dietary B12 for 4 to 6 weeks while still taking the supplement
- Taper gradually — if you’re on a daily supplement, reduce to every other day, then twice a week, then stop
- Recheck labs at 3 months and 6 months after stopping completely
- Monitor for symptoms — fatigue, tingling, numbness, brain fog, or mood changes should prompt immediate retesting
Remember, your liver stores enough B12 to last 3 to 5 years. This means you have a comfortable buffer — but it also means that if levels are dropping, you won’t feel it until stores are significantly depleted. Regular testing is the safety net.
An app like Gulpify can help you track your daily B12 intake from food, set reminders for lab retests, and monitor your adherence as you transition — so you’re not relying on memory alone.

Key Takeaways
- B12 deficiency is more common than you think — it’s not just a vegan concern. Age, medications, and gut health all play a role.
- The richest natural sources are shellfish, organ meats, and fish. Dairy and eggs provide B12 but in smaller amounts — you need to be intentional.
- Absorption matters as much as intake. Stomach acid, gut health, and medications like PPIs and metformin can quietly block B12 absorption.
- Spirulina and algae are not reliable B12 sources — they contain inactive analogues that your body can’t use.
- B12 doesn’t work in isolation. Deficiencies in vitamin D3, folate, and iron frequently overlap. Ask for the full panel, not just one test.
- High folate can mask B12 deficiency — always check B12 before supplementing folate.
- A “normal” serum B12 doesn’t always mean you’re fine. If your levels are in the gray zone (200-400 pg/mL) and you have symptoms, ask about methylmalonic acid (MMA) testing.
- Transitioning off supplements should be gradual and monitored with lab work at 3 and 6 months.
- Track what you eat. Whether you’re building up dietary B12 or tapering off a supplement, tracking your intake with a tool like Gulpify keeps you accountable and helps you spot gaps before they become deficiencies.
Sources
- NIH Office of Dietary Supplements. “Vitamin B12 — Fact Sheet for Health Professionals.” ods.od.nih.gov
- USDA FoodData Central. Nutrient data for B12 food sources. fdc.nal.usda.gov
- Green R et al. “Vitamin B12 deficiency.” Nature Reviews Disease Primers, 2017; 3:17040. doi:10.1038/nrdp.2017.40
- Stabler SP. “Vitamin B12 Deficiency.” New England Journal of Medicine, 2013; 368:149-160. doi:10.1056/NEJMcp1113996
- Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. National Academies Press, 1998. Link
- Andrès E et al. “Vitamin B12 (cobalamin) deficiency in elderly patients.” Canadian Medical Association Journal, 2004; 171(3):251-259. doi:10.1503/cmaj.1031155